
In the world of AI-driven health systems, two protocols dominate how agents operate: MCP (Model Context Protocol) and A2A (Agent-to-Agent Communication).
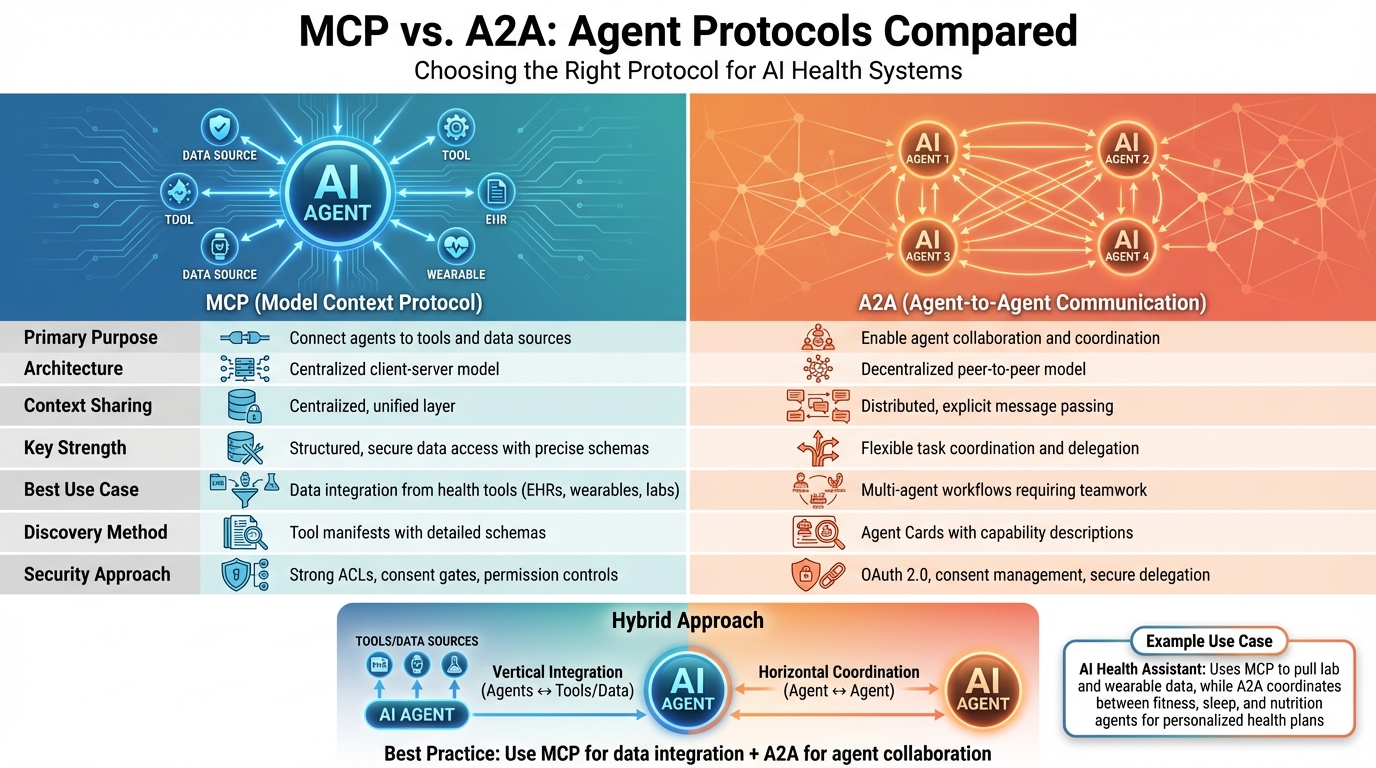
- MCP connects AI agents to tools and data sources like electronic health records (EHRs), wearables, and lab systems. It uses a centralized client-server model, ensuring secure, structured data access with precise schemas.
- A2A focuses on agent collaboration, enabling multiple agents to communicate and coordinate tasks through a decentralized peer-to-peer model. It uses "Agent Cards" to describe capabilities and supports workflows requiring teamwork.
Both protocols address different needs:
- MCP excels in integrating fragmented health data into a unified system.
- A2A is ideal for managing multi-agent task allocation and insights.
Together, they create a robust framework for health optimization, with MCP handling data integration and A2A managing collaboration. For example, an AI health assistant could use MCP to pull lab and wearable data, while A2A coordinates between agents like fitness or sleep coaches for a personalized health plan.
Quick Comparison
| Feature | MCP (Model Context Protocol) | A2A (Agent-to-Agent Communication) |
|---|---|---|
| Purpose | Connect agents to tools and data | Enable agent collaboration |
| Architecture | Centralized client-server | Decentralized peer-to-peer |
| Context Sharing | Centralized, unified layer | Distributed, explicit message passing |
| Key Strength | Structured, secure data access | Flexible task coordination |
| Best Use Case | Data integration from health tools | Multi-agent workflows and collaboration |
For health optimization, MCP ensures agents access reliable data, while A2A enables them to work together effectively. Systems like BondMCP leverage MCP for unified health data, making it easier for agents to deliver actionable insights while adhering to U.S. regulations like HIPAA.
MCP vs A2A Protocol Comparison for Health AI Systems
AI Agent Protocols Explained: MCP, A2A, ACP and More
What is MCP (Model Context Protocol)?
The Model Context Protocol (MCP), developed by Anthropic, is a standardized framework designed to help AI agents easily connect with external tools, data sources, and services. Think of it as a universal connector that allows health-focused AI systems to seamlessly interact with wearables, electronic health records, lab databases, or even supplement tracking apps.
MCP operates using a client–server setup. In this system, the AI agent acts as the client, requesting data or services from tools and systems that act as servers. For example, a fitness coaching AI might use MCP to gather sleep patterns, lab test results, or supplement tracking data through standardized, consistent connections.
At its core, MCP relies on JSON-RPC 2.0 for structured request–response interactions, with optional real-time updates supported through Server-Sent Events (SSE). When an AI agent needs specific information, it sends a request formatted to MCP's specifications. The response is returned in a predictable, schema-defined structure, ensuring clarity and consistency.
One of MCP's standout features in healthcare is its focus on security and permissions. Each connection enforces strict access controls, specifying exactly what data can be accessed and what actions are allowed. This is particularly important for compliance with regulations like HIPAA in the U.S. Additionally, MCP organizes tasks as individual function calls with clear inputs and outputs, rather than relying on complex, stateful processes. This approach simplifies development and ensures reliable interactions between AI agents and health tools.
Core Features of MCP
Several key components make MCP a powerful framework for secure and standardized communication between agents and tools:
- Context Objects: These provide a structured, shared view of the data relevant to an AI agent's tasks. For example, a blood glucose reading is consistently formatted across all systems, thanks to strict schemas.
- Tool Definitions: Each tool specifies its capabilities through a manifest. This includes functions, required inputs, outputs, and any constraints. For instance, a lab tool might offer functions like
getLatestCBC()orgetTrendingBiomarkers(timeframe), allowing agents to dynamically discover and use these capabilities. - Schema-Driven Inputs and Outputs: By enforcing precise data formats, MCP eliminates the ambiguities that often arise in traditional API integrations.
- Transport Patterns: MCP supports both standard HTTP request–response interactions and real-time streaming via SSE. This flexibility enables everything from continuous monitoring to batch data retrieval.
How MCP Works in Health Agent Orchestration
In health optimization, MCP acts as the glue that brings together data from multiple fragmented sources into one cohesive system. Wearable devices, glucose monitors, lab services, and health apps all share their data through MCP's standardized connections. This unified approach ensures that AI agents can gather and process diverse health data in a consistent format, enabling timely and data-driven health interventions. For instance, an agent might automatically adjust a user's activity recommendations based on new biometric data.
BondMCP: A Specialized Version for Health Optimization
Building on MCP's foundation, BondMCP tailors the framework specifically for personal health optimization. It addresses the unique challenges of integrating and managing diverse health data, positioning itself as "the missing intelligence layer in the fragmented world of personal health optimization."
BondMCP enhances the standard MCP framework by incorporating a health-specific ontology - a standardized vocabulary and data model. This ensures consistency in how health metrics are defined and interpreted. For example, "sleep quality" is represented uniformly, whether the data comes from a wearable device or a clinical study.
BondMCP creates a unified health model that provides a comprehensive, real-time view of an individual’s health. This includes current biomarkers, ongoing interventions, health goals, and historical trends. Developers benefit from an SDK and structured protocols that simplify the creation of health-aware AI agents, removing the need to build complex systems for memory management or tool integration from scratch. For users, the result is a smooth experience: their sleep tracker can inform their fitness coach, lab results can adjust their supplement plan, and longevity goals can guide real-time decisions - all working together seamlessly in the background.
With over 2.5 million API calls handled monthly, a 99.9% uptime, and an average response time of 1.8 seconds, BondMCP has become a trusted solution for more than 50 health systems and 12,000 active developers worldwide[1]. It’s setting a new benchmark for agent-driven health optimization.
What is A2A (Agent-to-Agent Communication)?
Agent-to-Agent (A2A) communication is a standardized protocol that allows AI agents to directly connect, exchange messages, and collaborate on tasks. Unlike MCP, which focuses on linking agents to tools and data sources, A2A emphasizes peer-to-peer collaboration. This setup enables specialized agents to tackle complex tasks together by delegating responsibilities, sharing insights, and coordinating their efforts.
A2A is built as a general-purpose messaging framework that can be applied across various fields. It’s being developed by a community led by Google and other collaborators to establish a neutral standard for interoperability between agents. This means agents created by different vendors or teams can work together seamlessly, as long as they adhere to the A2A protocol.
The A2A model organizes tasks into distinct states, such as submitted, working, input-required, completed, or failed. This structure is ideal for managing long-running workflows, including those requiring human approvals. For instance, in a U.S. health system, a prior authorization process might involve multiple agents working over several days, each contributing updates as the task progresses. This task-oriented design is key to understanding how A2A can streamline health workflows.
A2A relies on Agent Cards, which are standardized JSON metadata documents. These cards describe an agent’s capabilities in broad terms, such as "can interpret ECG data" or "can verify insurance benefits", along with details about supported communication channels and security protocols. This setup allows agents to dynamically identify and collaborate with the right partners for specific tasks, even in complex environments involving multiple agents.
The protocol supports various interaction patterns, including synchronous, streaming, and asynchronous communication. Security is a priority, with requirements for OAuth 2.0, consent management, and secure delegation.
How A2A Works in Health Agent Systems
In healthcare, A2A facilitates coordination among specialized agents to manage patient workflows while maintaining accountability. For example, if a wearable device detects an abnormal heart rate, it could trigger a cardiac assessment task. This task might then cascade into sub-tasks, such as consulting cardiology guidelines or scheduling urgent care, all managed through A2A messaging.
This framework supports different types of communication, including:
- Direct messaging: One agent sends structured data to another.
- RPC-like calls: An agent requests a specific capability, such as scheduling a follow-up appointment by providing a patient ID and preferred time slots.
- Event-driven exchanges: Agents publish events like "lab_result_ready", which can trigger downstream actions.
These mechanisms enable flexible, loosely connected workflows where agents from different vendors or teams can collaborate effectively, as long as they follow the A2A standard.
A2A’s stateful task model is particularly useful for workflows requiring human-in-the-loop approvals or those that span multiple clinical interactions. For instance, a chronic disease management program might involve a 30-day care plan where agents coordinate tasks related to nutrition, medication, and exercise. Periodic check-ins and adjustments based on patient progress and clinician input can be seamlessly integrated into this framework.
Limitations of A2A in Health Orchestration
While A2A is effective for agent collaboration, it has notable limitations when used independently for health orchestration.
First, A2A doesn’t standardize how agents connect to external tools, databases, or APIs. Each agent must build its own integrations to access systems like EHRs, lab databases, or wearable devices. This results in duplicated efforts and inconsistencies in how data is accessed and interpreted.
Second, the high-level capability descriptions in Agent Cards lack detailed schemas for function calls. For example, while an Agent Card might state that an agent "can analyze lab results", it doesn’t specify the exact input format, required parameters, or expected output. This lack of detail makes precise and predictable interactions more challenging - an issue that’s particularly critical in clinical decision-making, where ambiguity can lead to errors.
Another major challenge is the absence of secure agent memory protocols to provide a unified context layer. In A2A, context must be explicitly passed between agents through tasks and messages, rather than being maintained in a shared, consistent state. This can lead to fragmented context, where agents operate with incomplete or outdated information. For instance, if a patient’s medication list changes, each agent that relies on this information must be updated individually through separate A2A messages. In a U.S. healthcare setting, this fragmentation increases the risk of clinical errors and complicates compliance with HIPAA regulations, which require consistent access controls and audit trails for all systems handling protected health information (PHI).
As the number of agents grows, managing individual connections, permissions, and audit trails becomes increasingly complex. Without a higher-level orchestration layer, ensuring accountability and meeting regulatory requirements can become a significant burden for developers and compliance teams.
These limitations highlight why A2A alone may lead to fragmented workflows in healthcare, underscoring the importance of integrating robust context layers like those provided by MCP.
sbb-itb-f5765c6
MCP vs. A2A: Direct Protocol Comparison
Architecture and Abstraction Differences
When it comes to their underlying structures, MCP and A2A take very different approaches. MCP relies on a centralized client-server model, where a single agent connects to external tools and data sources using standardized protocols. This setup ensures clear communication through well-defined tool manifests, which specify precise input and output schemas - an approach that minimizes ambiguity, especially in clinical settings.
A2A, on the other hand, adopts a decentralized, peer-to-peer model. Agents in this system discover and communicate with one another using Agent Cards. These JSON-based documents outline an agent's capabilities in broad terms - for example, an agent might handle ECG interpretation or verify insurance benefits. While MCP provides explicit instructions for function calls, A2A focuses on high-level descriptions, leaving the finer details to be worked out during runtime.
Context Management and Task Allocation Differences
The two protocols also diverge significantly in how they handle context and assign tasks. MCP centralizes context management, creating a unified layer where all data - such as lab results, fitness metrics, or supplement plans - exists in a validated and secure state. This centralized approach allows agents to access shared information under strict permissions, ensuring both security and consistency. For example, systems like BondMCP leverage this model to streamline interactions in health contexts.
In contrast, A2A distributes context management across agents. Each agent is responsible for maintaining its own state and explicitly updating others when changes occur. For instance, if a patient's medication list is updated, every relevant agent must be notified individually. While this distributed model supports flexible collaboration among agents, it also introduces challenges in maintaining consistency. A2A’s task model, which includes phases like "submitted", "working", and "input-required", is particularly effective for managing long-running workflows, but it lacks the centralized context layer that MCP uses to simplify operations and ensure compliance.
MCP vs. A2A Comparison Table
| Dimension | MCP (Model Context Protocol) | A2A (Agent-to-Agent Protocol) |
|---|---|---|
| Primary Purpose | Connect agents to tools, APIs, and data sources | Enable agents to discover and collaborate |
| Architecture Style | Centralized client-server | Decentralized peer-to-peer |
| Work Model | Individual function calls with precise schemas | Manages task lifecycles (e.g., submitted, working) |
| Context Sharing | Centralized with detailed permissions | Distributed, requiring explicit message passing |
| Task Allocation | Centralized routing with session management | Distributed negotiation and delegation |
| Discovery Mechanism | Uses tool manifests | Relies on Agent Cards |
| Security & Compliance | Strong ACLs, consent gates, and permission controls | OAuth 2.0, consent management, secure delegation |
| Scalability | Ideal for single-agent tool access | Optimized for multi-agent workflows |
| Suitability for Health | Best for structured data integration and orchestration | Best for coordinating specialized health agents |
This breakdown highlights the strengths of each protocol. MCP shines in scenarios requiring secure, structured access to external systems, while A2A thrives in coordinating multiple agents for collaborative tasks. In many cases, these protocols can work together - MCP handling the tools and data integration, while A2A facilitates dynamic teamwork among agents.
Designing Health Agent Systems with MCP and A2A
Combining MCP and A2A in Hybrid Systems
Hybrid systems bring together MCP (Meta-Cooperation Protocol) for vertical tool integration and A2A (Agent-to-Agent) communication for horizontal coordination. Here’s how it works: MCP connects each agent to its designated tools and data sources - think wearable APIs, lab databases, or supplement registries. Meanwhile, A2A enables agents to find each other, share information, and delegate tasks efficiently.
For example, a meta-agent tasked with "optimizing cardiovascular health" could break this goal into smaller, specialized tasks. Nutrition agents might analyze dietary habits, fitness agents could focus on exercise routines, and sleep agents would monitor rest patterns. Using MCP, these agents securely pull data from external sources like food databases, wearable devices, or sleep trackers. The meta-agent then combines these insights into a comprehensive health plan.
This modular design allows each agent to operate independently while still working toward shared health goals. A great example of this is BondMCP’s shared context layer, which ensures health data is normalized and validated across the board. These principles align with the high standards required in the US health system, ensuring both flexibility and reliability.
US Health System Requirements
The US health system imposes strict regulations, especially around HIPAA compliance, requiring features like encryption, audit trails, and explicit patient consent. MCP addresses these needs with fine-tuned permissions and access controls for tools and data. At the same time, A2A ensures secure agent authentication, often using OAuth 2.0 and detailed security declarations embedded in agent profiles.
Additionally, US systems rely on imperial units - temperature in °F, weight in pounds, and height in feet/inches. They also demand precise reporting of key health metrics like blood pressure (mmHg), cholesterol (mg/dL), and glucose levels (mg/dL) to avoid errors during unit conversions.
BondMCP is designed with these US-specific needs in mind. Its health-focused ontology incorporates customary units and essential metrics like VO2 max, HRV, and sleep stages. The platform also ensures HIPAA compliance with enterprise-grade security measures, including detailed audit trails and patient consent tracking that logs which agents accessed specific data. BondMCP exemplifies the scalability and rigor needed for health optimization platforms in the US, meeting both technical and regulatory demands seamlessly. [1]
Conclusion: Selecting the Right Protocol for Health Optimization
When it comes to MCP and A2A, it's not an either-or decision - each protocol plays to its strengths. MCP is your go-to for vertical integration, giving individual agents streamlined access to tools, APIs, and health data sources like electronic health records (EHRs), wearables, and lab systems. On the other hand, A2A is built for horizontal collaboration, enabling multiple agents to work together on complex, long-term workflows that may take weeks or even months.
For a comprehensive approach to health optimization, the strategy is straightforward: start with MCP to ensure consistent access to tools and data, and layer in A2A when you need agents to collaborate on intricate care plans. For instance, a single health assistant pulling data from a wearable and lab portal can function seamlessly with MCP. However, a longevity program managing nutrition, exercise, sleep, and diagnostics over an extended period benefits greatly from A2A’s ability to handle task lifecycles and inter-agent communication.
BondMCP simplifies this process by offering a tailored implementation of MCP. Instead of creating context-aware health agents for every data source, BondMCP provides a shared context layer with a health ontology. This standardizes data such as lab values (mg/dL), wearable metrics (like HRV and VO2 max), supplements, and lifestyle information, making it easier to work with.
The real power of BondMCP lies in eliminating fragmented data and siloed agents. By unifying health signals, it ensures all agents operate from the same consistent dataset rather than conflicting or incomplete snapshots. For clinics, platforms, and biohackers in the U.S., this translates to greater clarity, personalization, and scalable automation.
FAQs
How does MCP protect data and comply with regulations like HIPAA?
BondMCP places a strong emphasis on data security and staying compliant with regulations by employing top-tier healthcare security protocols. These measures include SOC 2 Type II certified controls, end-to-end encryption, multi-factor authentication, API key management, and comprehensive audit logging.
With these protections in place, sensitive data stays secure while adhering to strict standards like HIPAA. This approach ensures confidence for both users and developers when handling critical information.
What are the key challenges of using A2A protocols for health-focused agent collaboration?
A2A (Agent-to-Agent) protocols encounter significant hurdles when applied to health-focused agent collaboration, largely due to the fragmented and complex nature of health data. One of the primary challenges is the absence of a unified context layer. Without this, agents struggle to interpret and share information effectively across varied sources like wearables, lab results, and fitness apps.
Interoperability is another major obstacle. Many A2A systems fail to ensure smooth collaboration between agents, especially when navigating diverse health ontologies and the tailored needs of personalized care. This lack of cohesion often results in redundant tools, disjointed user experiences, and limited automation - ultimately hindering the ability to improve health outcomes through collaboration.
To overcome these barriers, a protocol must be developed that supports context-aware, interoperable, and health-literate communication between agents. This would pave the way for a more seamless and personalized health ecosystem.
What are the differences between MCP and A2A, and how can they work together in health agent systems?
MCP (Model Context Protocol) and A2A (Agent-to-Agent) protocols are both key to facilitating communication between AI agents, though they address different needs. MCP is designed to establish a shared context layer, ensuring agents can work together effectively, remain context-aware, and process domain-specific data like health information. Meanwhile, A2A focuses on enabling direct communication between agents, making it possible for them to exchange information and collaborate smoothly.
When integrating MCP and A2A in health agent systems, MCP lays the groundwork by creating a unified structure and shared understanding for interpreting health-related data. A2A complements this by enabling real-time collaboration between agents. This combination can bring together scattered data from wearables, lab results, and fitness devices, forming a unified system that automates and personalizes health management.